Are you able to… (mark Yes for each that the patient can perform)
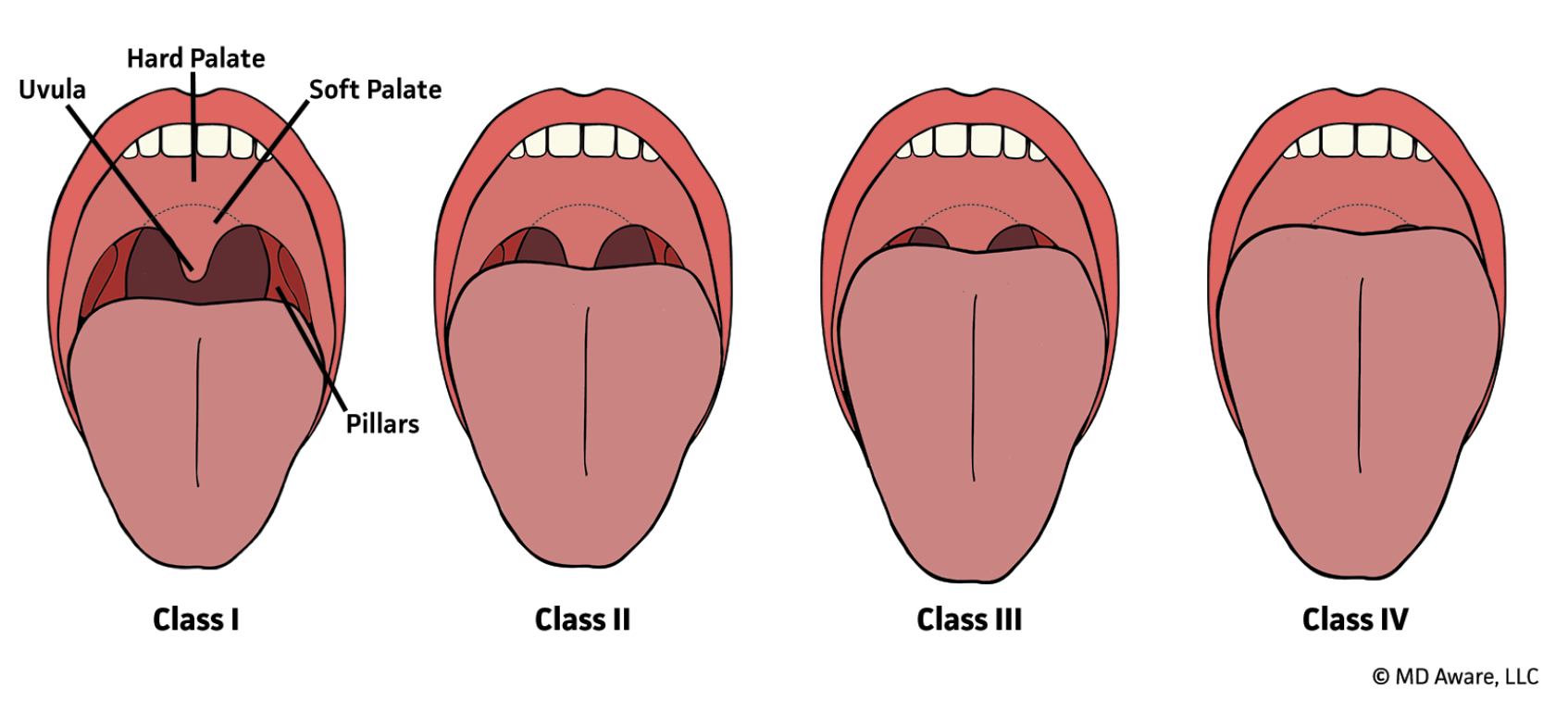
Faucial pillars, soft palate, and uvula visualized
Faucial pillars and soft palate visualized, but uvula masked by tongue base
Only soft palate visualized
Soft palate not visualized
This number is the objective SORT score only (the published 2014 model). It does not include the clinician's own estimate that SORT v2 adds. Any estimate you pick above is saved in the note next to this score, not mixed into it.
Paste the Patient's Active Medication List.
Spelling Matters. The tool checks each line against an expanded drug dictionary, so a misspelled, abbreviated, or oddly written name may not be recognized.
One Medication Per Line. The tool references an expanded drug dictionary, so a misspelled, abbreviated, or oddly written name may not be recognized. Anything it cannot match is listed under “Unclassified: Manual Review.” Both brand and generic names are accepted.
Everything runs in your browser. No information is recorded or stored. Include: 1) Medication Name, with or without the dose 2) Date of Last Dose Taken.
Assessment Template0/15 sections complete
Copy and paste into the PAT note. Edit as appropriate.
Educational reference only. Not clinical decision support. The generated text is a starting point; the responsible clinician edits per clinical judgment, institutional policy, and current guidance.
Perioperative Risk Summary
Snapshot of calculator outputs entered above, in order of workflow. Educational reference; defer to local protocol and judgment.
| Calculator | Result / Output | Risk interpretation & summary |
|---|
Medication Reconciliation & Recommendations
Recommendations reflect common perioperative guidance tied to procedure date and are educational. Final hold/continue decisions defer to the attending and institutional protocol.
| Medication / class | System / category | Reconciliation status / finding | Recommendation & timing |
|---|
No medications entered yet. Paste a list on the Medication Reconciliation tab (and complete the SGLT2i tab if relevant) to populate this table.